Vocal fold regeneration is a difficult repair problem because the tissue does more than close a wound. It has to function as a moving tissue, not just a healed surface. The vocal fold needs a compliant, layered structure that deforms with airflow, springs back, and keeps vibrating cycle after cycle. Scar-like stiffness is basically the failure mode. That means a regenerated vocal fold cannot be judged by histology alone.
A recent paper in Stem Cell Research & Therapy tested this in a rabbit vocal fold scar model using a PEG-fibrin hydrogel and mesenchymal stromal cell spheroids. The comparison was clean: PEG-fibrin alone versus PEG-fibrin with MSCs delivered as a suspension versus PEG-fibrin with MSC spheroids after scar excision.
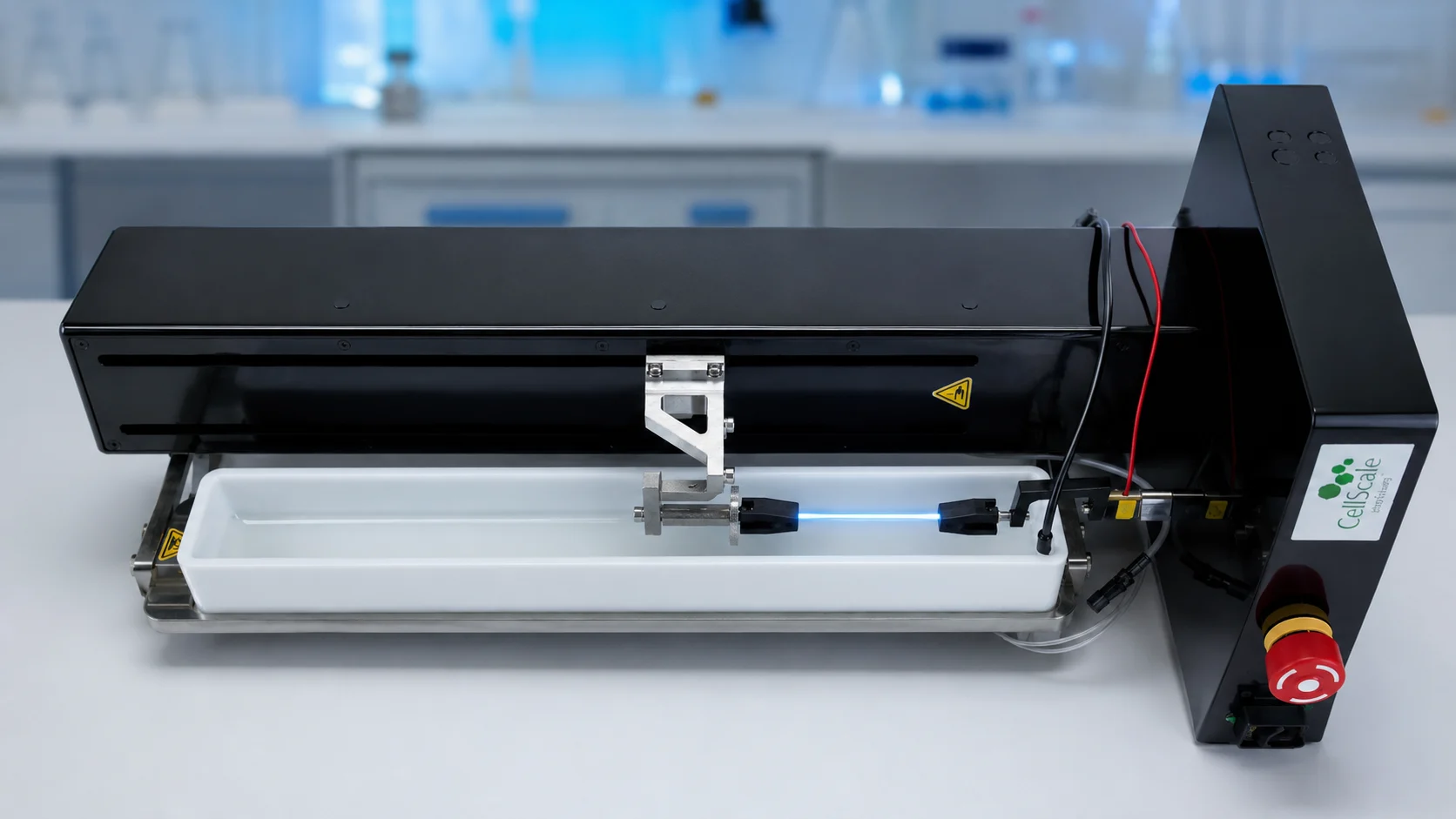
The CellScale MicroTester was used in the study to measure local vocal fold stiffness by indentation testing, giving the team a way to compare treated tissue with intact vocal fold tissue.
What makes the study useful from a mechanical testing perspective is the way it links tissue repair to function-related measurements. The researchers followed cell behaviour, histological structure, lamina propria thickness, local Young’s modulus, and vibration activity.
The question running through the work was fairly practical: after treatment, does the scarred vocal fold start to look and behave more like native tissue? A good insight into vocal fold regeneration.
Why Vocal Fold Regeneration Is Also a Mechanics Problem
A scarred vocal fold is not just “injured.” The lamina propria reorganizes, thickness can shift, and the tissue often ends up mechanically different from native fold, especially in stiffness. Those changes matter because vibration is the job. If the fold cannot deform and rebound the right way, voice outcomes stay limited even when the surface looks healed.
That is why MSC-based strategies keep coming up in this space. The goal is not simply to add cells, but to steer the local repair environment through paracrine effects, including how inflammation resolves and how matrix remodeling and fibrosis unfold. In practice, though, cell retention is a persistent problem. If injected cells do not remain at the defect site long enough, their local effects may be short-lived.
That is where MSC spheroids become interesting. A spheroid is a small 3D cell aggregate with cell-cell contacts and its own developing extracellular matrix. Compared with a dispersed cell suspension, spheroids may retain cells more effectively and may change how those cells behave once delivered into a hydrogel or tissue defect.
This work also fits into a broader trend toward spheroid-based repair strategies, including studies using injectable scaffolded spheroids for nucleus pulposus regeneration.
Building a PEG-Fibrin Bioequivalent with MSC Spheroids
The researchers used human mesenchymal stromal cells derived from alveolar mucosa of the gum. The cells were formed into spheroids using non-adhesive agarose plates, with 2,000 cells seeded per spheroid. Over several days, the cells aggregated and compacted into rounded microtissues.
The spheroids were then combined with a PEG-fibrin hydrogel system. The hydrogel acted as a carrier for implantation, while the spheroids provided a more structured form of cell delivery than a conventional MSC suspension. The study compared this spheroid-based bioequivalent against PEG-fibrin alone and PEG-fibrin containing dispersed MSCs.
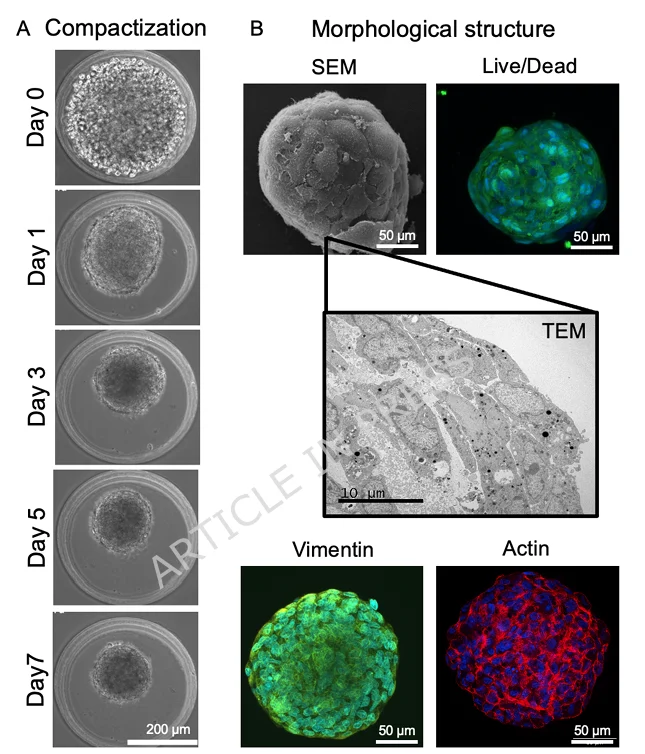
One detail that stands out is that the spheroids did not remain inert inside the hydrogel. In PEG-fibrin, cell outgrowths began to appear after 24 hours, and by day 7 the sprouts had extended several hundred micrometres. That matters because the hydrogel was not only being used as a filler. It was part of the local environment where the cells had to survive, spread, and interact with the surrounding tissue.
Testing Vocal Fold Regeneration in a Rabbit Scar Model
The central in vivo vocal fold regeneration experiment used a rabbit model of mature vocal fold scarring. The researchers first created a unilateral injury in the left vocal fold and allowed the scar to mature for 3 months. Then they excised the scarred area to create a secondary defect and injected one of four treatments:
- No treatment control
- PEG-fibrin without cells
- PEG-fibrin with MSC suspension
- PEG-fibrin with MSC spheroids
Intact vocal folds were also analyzed for comparison.
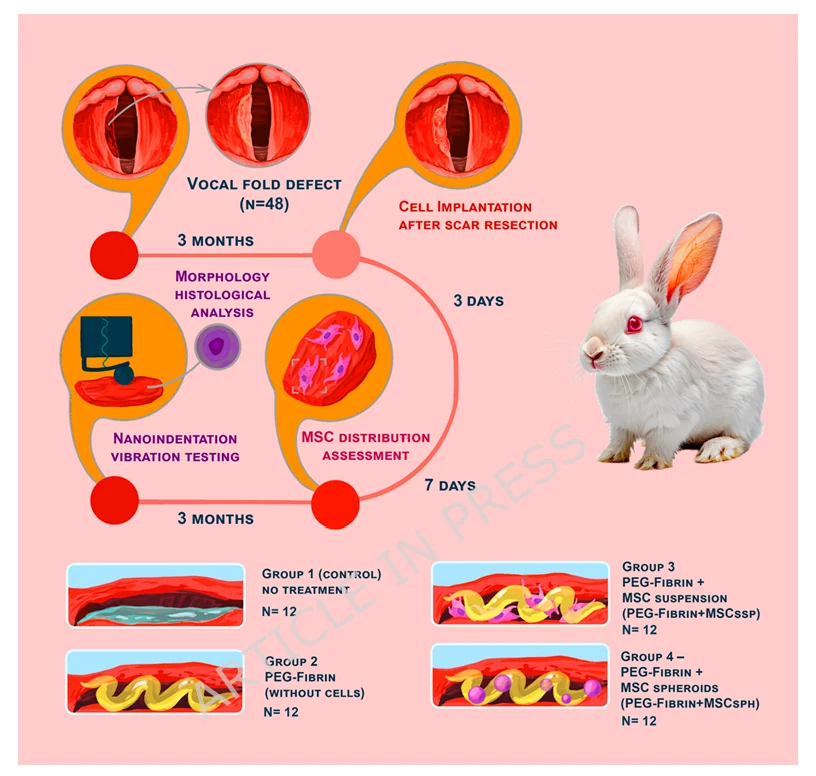
This design is useful because the researchers were not only looking at acute wound closure. They created a scar, waited for it to mature, then tested whether the secondary repair process could be altered by different PEG-fibrin based implants. That makes the work more relevant to vocal fold scar regeneration than a simple fresh injury model.
Using the MicroTester for Vocal Fold Mechanical Testing
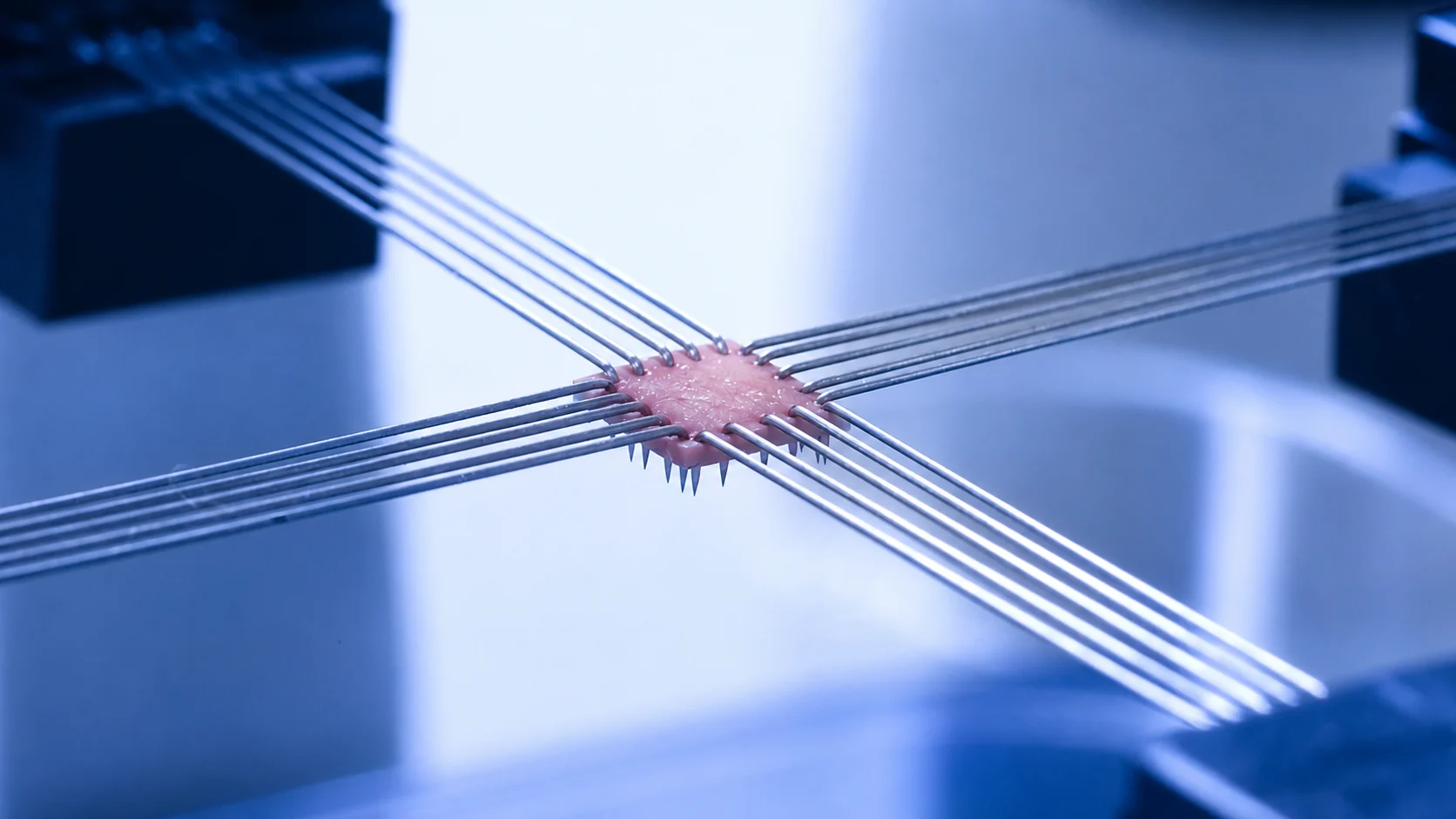
For the mechanical testing part of this vocal fold regeneration study, the dissected samples were placed in PBS and immobilized on glass slides. The researchers used a MicroTester G2 in indentation mode, measuring each sample three times. A spherical microindenter with a diameter of 1.5 mm was attached to a tungsten beam, and the samples were indented to a depth of 800 µm.
The resulting force-displacement data were analyzed using a Hertz model to calculate Young’s modulus. This gave the researchers a local stiffness measurement for each treated vocal fold, which could then be compared with intact tissue from the same experimental context.
This is a useful way to think about vocal fold regeneration and stiffness. The tissue is small, soft, hydrated, and mechanically delicate. A bulk tensile test would not capture the same local behaviour in the lamina propria region. Indentation gave the authors a way to probe the repaired tissue in a hydrated state and compare local mechanical behaviour across groups.
For researchers working with other small or irregular biological samples, we have also discussed how micro-scale testing can be used to measure forces and stiffness in cell clusters and soft tissue constructs.
What Changed After 3 Months?
By the three-month mark, the groups separate in a way that is hard to miss, both in tissue appearance and in how “scar-like” the lamina propria remains.
The untreated scar group looks like a classic fibrotic outcome. The untreated scar group shows the most obvious fibrotic outcome. The defect area is described as thickened at the surface, with dense connective tissue underneath and extensive inflammatory involvement. Vascularity is increased and fibrosis reaches into the muscle. The lamina propria is much thicker than intact tissue, at about 322 µm.
PEG-fibrin alone closes the surface, but the deeper layer still reads as scar-like. The epithelium is continuous, yet the subepithelial region remains compact and collagen-rich. Lamina propria thickness stays elevated (about 274 µm), and collagen is still tightly organized.
With MSCs delivered as a suspension, the tissue looks less inflamed and the matrix appears looser. The epithelium is more mature, and immune-cell presence is reduced compared with the untreated scar. The lamina propria is improved but still above intact levels, around 180 µm.
The strongest “near-native” pattern shows up in the MSC spheroid condition. The mucosa is described as mature stratified squamous epithelium without obvious dystrophic features, and the subepithelial connective tissue is looser with more longitudinal collagen organization and only mild lymphocyte/macrophage infiltration. The lamina propria is about 116 µm, and this is the only treatment group reported as not different from intact tissue on thickness.
They also use α-SMA staining as a fibrosis readout. In the untreated scar tissue, α-SMA positive myofibroblasts are abundant and align with collagen fibres. In the MSC spheroid group, α-SMA signal is reported mainly in vascular smooth muscle (and partly in epithelium), which is closer to the distribution seen in normal vocal fold tissue.
Vocal Fold Stiffness After MSC Spheroid Treatment
The MicroTester data helped connect the tissue-level observations to local mechanics.
In the untreated group, scarred vocal fold tissue was stiffer than intact tissue. The reported Young’s modulus was about 6.63 kPa for scarred tissue compared with 3.35 kPa for intact tissue. That is roughly a 1.9-fold increase in stiffness.
The PEG-fibrin only group did not show a statistically significant difference between treated and intact tissue. The values were about 4.73 kPa for treated tissue and 4.08 kPa for intact tissue.
The MSC suspension group was more variable and, somewhat unexpectedly, the treated tissue was stiffer than intact tissue. The authors reported about 5.60 kPa for treated vocal folds compared with 2.23 kPa for native tissue. They suggested that the variability may reflect heterogeneous vocal fold regeneration or uneven tissue remodelling.
The MSC spheroid group showed a different pattern. Treated and intact tissue had similar Young’s modulus values, about 4.13 kPa and 3.19 kPa, respectively, with no significant difference between them.
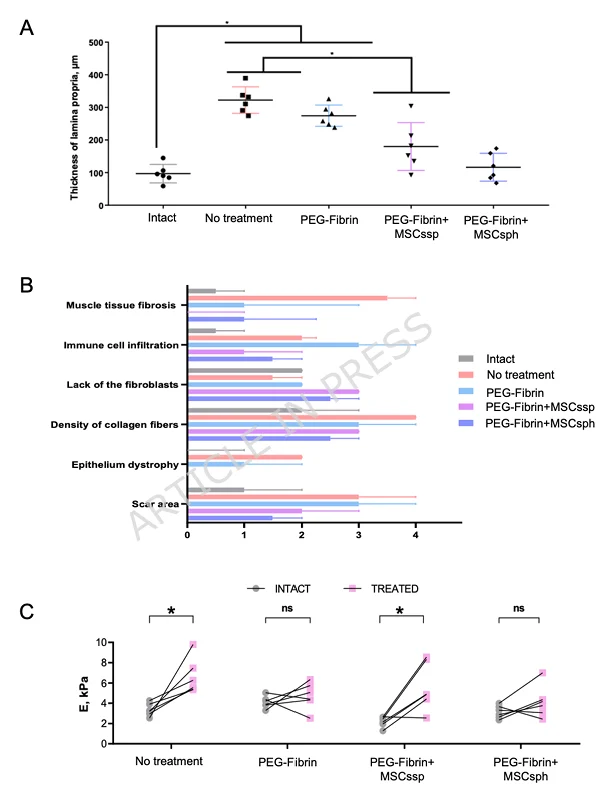
One thing to be careful about is that PEG-fibrin alone also produced Young’s modulus values that were not significantly different from intact tissue. So the study should not be read as saying that only MSC spheroids restored stiffness. The more useful observation is that the spheroid group had the best combined profile: more native-like lamina propria thickness, looser tissue architecture, lower scar-related features, and local stiffness that was not significantly different from intact vocal fold tissue.
Vibration Behaviour Was Also Checked
The researchers also measured vocal fold vibration using a non-contact optical setup. This was separate from the CellScale testing. They recorded vibration frequency ranges while airflow was applied to the samples and compared the treated vocal folds with intact tissue.
Across the fibrin-based treatment groups, the authors did not find significant differences in the fundamental frequency ranges compared with intact tissue. For the MSC spheroid group, the treated and intact values were especially close across the measured frequency bands.
Vocal fold regeneration has to be understood across several scales: histological structure, local stiffness, and vibration behaviour. A tissue that looks repaired but cannot move properly would still be functionally incomplete.
Why MSC Spheroids May Have Helped
The authors suggest that MSC spheroids may support vocal fold regeneration partly because they improve cell retention at the defect site. Human cell staining showed implanted cells near the gel residue at day 3 and within newly formed granulation tissue at day 7. In the spheroid group, positively stained cells appeared more prominent than in the MSC suspension group.
That retention matters if the main value of MSCs is what they release rather than what they become. Keeping the cells clustered as spheroids may help them persist through the early post-injury window and may shift the mix or timing of signals they put out. A spheroid is also a different starting state than a dispersed suspension, with cell-cell contact already established and a local matrix beginning to form. The PEG-fibrin hydrogel then provides a carrier environment that keeps the cell aggregates at the injury site during early tissue remodelling.
It is still an association in one animal model, not a straight line to the clinic. But the pattern is instructive: the spheroid condition aligns with a more “near-native” outcome in both structure and stiffness-related readouts. And it reinforces a broader point about vocal fold repair studies, where mechanical testing helps show whether tissue remodeling is moving toward function, not just a nicer histology slide.
Measuring Soft Tissue Repair with the MicroTester
In this study, the MicroTester was used to indent vocal fold samples in PBS and calculate local Young’s modulus. That type of measurement is useful when researchers need to compare small, soft, hydrated biological tissues without relying only on gross visual changes or histological scoring.
The MicroTester is often used for mechanical testing of small biological samples, soft materials, hydrogels, engineered tissues, cell aggregates, and other specimens where local force and displacement measurements are needed. In a workflow like this one, the instrument gives researchers a practical way to ask whether a repaired tissue is mechanically closer to native tissue.
For vocal fold regeneration, that question matters. The treated tissue has to rebuild the right kind of extracellular matrix, but it also has to recover a mechanical behaviour that supports vibration. By pairing MicroTester indentation with histology and vibration measurements, the authors were able to look at the repair process from more than one angle.
The study is a good reminder that regenerated tissue is not only something to see under a microscope. It is something that has to move, deform, and respond mechanically in a way that fits its job.
Citation
Shpichka, A., Svistushkin, M., Khristidis, Y. et al. SPHERpower: MSC spheroid-based bioequivalent lead to the efficient restoration of the scarred vocal folds. Stem Cell Res Ther (2026). https://doi.org/10.1186/s13287-026-05067-5